Introduction
Physiotherapy in Vernon for Wrist and Forearm Issues
Welcome to Vernon Physiotherapy & Rehab’s resource about intersection syndrome.
Intersection syndrome is a painful condition of the forearm and wrist. It can affect people who do repeated wrist actions, such as weight lifters, downhill skiers, and canoeists. Heavy raking or shoveling can also cause intersection syndrome.
This guide will help you understand:
- what part of your forearm is causing the problem
- what may have caused this condition
- how health care professionals diagnose it
- what can be done to stop the pain
- what is Vernon Physiotherapy & Rehab’s approach to rehabilitation
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Hand Pain|limit:15|heading:Hear from some of our patients who we treated for *Hand Pain*#
Anatomy
What part of the forearm is causing my pain?
The pain from intersection syndrome is usually felt on the top of the forearm, about three inches above the wrist. At this spot, two muscles that connect to the thumb cross over (or intersect) the two underlying wrist tendons (tendons connect muscles to bones).
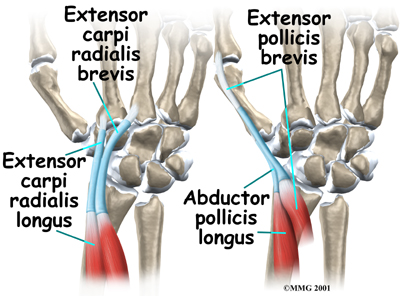
The two muscles that cross over the wrist tendons control the thumb. They are the extensor pollicis brevis and the abductor pollicis longus. These two muscles start on the forearm, cross over the two wrist tendons, and connect on the back part of the thumb. When these muscles work, they pull the thumb out and back.
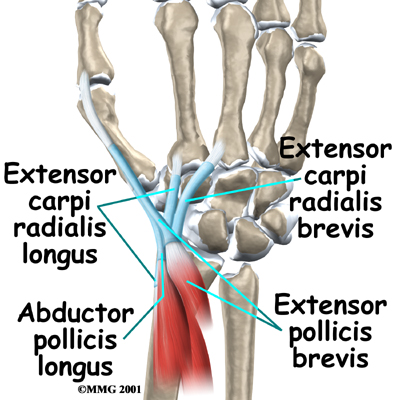
The extensor carpi radialis brevis and the extensor carpi radialis longus muscles run lengthwise along the back of the forearm. The tendons of these two muscles attach on the back of the hand. The action of these two wrist tendons pulls the wrist back, into extension.
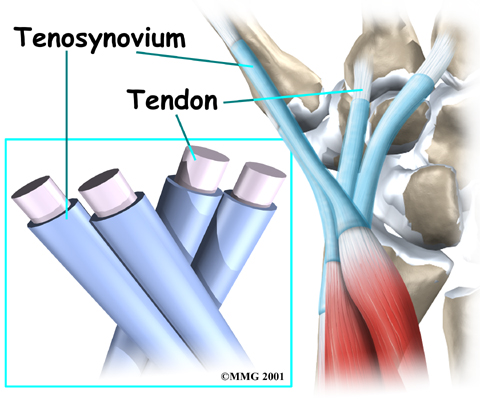
Most of the tendons around the wrist are covered with a thin tissue called tenosynovium. Tenosynovium is very slippery. It allows tendons to glide against one another and the surrounding muscles, fat, and skin with very little friction.
Causes
What caused my condition?
If you overuse the wrist extensor tendons, the slippery tenosynovial lining may become inflamed from the constant rubbing against the two thumb muscles. As the tenosynovium becomes more irritated and inflamed, it swells and thickens. You feel pain when you move your wrist because the swollen tendons are rubbing against the thumb muscles.
Wrist extensor tendons work like the bow used by violin players. The wrist extensor tendons are like the bow, and the thumb muscles are like the strings. As the wrist curls down and in, the wrist tendons rub back and forth against the thumb muscles. The friction builds up, much like the effect of rubbing two sticks together. This can lead to irritation and inflammation of the tenosynovium covering the wrist extensor tendons.
The wrist extensor tendons are strained by any activities that cause the wrist to curl down and in, toward the thumb. These wrist movements are especially common in downhill skiers when they plant their ski poles deeply in powder snow. The same movement is involved when pulling a rake against hard ground. Racket sports, weight lifting, canoeing, and rowing can also stress the wrist extensor tendons.
Symptoms
What does intersection syndrome feel like?
The friction on the wrist tendons causes pain and swelling in the tenosynovium that covers the tendons. The friction hampers the smooth gliding action. You may hear a squeaking sound and feel creaking as the tendons rub against the muscles. This is called crepitus. You may have swelling and redness at the intersection point. Pain can spread down to the thumb or up along the edge of the forearm.
Diagnosis
Diagnosis begins with a complete history. Your physiotherapist at Vernon Physiotherapy & Rehab will ask questions about where precisely the pain is, when the pain began, what you were doing when the pain started, and what movements aggravate or ease the pain.
 Next we will do a physical examination. We will palpate all around the wrist to determine you most tender point. We will also look for swelling or redness in the area. Next we will check the strength of your muscles around the wrist, elbow, and hand. We may ask you to resist certain movements while checking for pain or discomfort. We may even do a grip strength test to determine if your condition has caused you to lose some of your strength and to get a baseline measure so we can easily track your improvement with rehabilitation.
Next we will do a physical examination. We will palpate all around the wrist to determine you most tender point. We will also look for swelling or redness in the area. Next we will check the strength of your muscles around the wrist, elbow, and hand. We may ask you to resist certain movements while checking for pain or discomfort. We may even do a grip strength test to determine if your condition has caused you to lose some of your strength and to get a baseline measure so we can easily track your improvement with rehabilitation.
Usually we can make the diagnosis of intersection syndrome just from your history and during the physical examination; most of the time no special diagnostic tests are required.
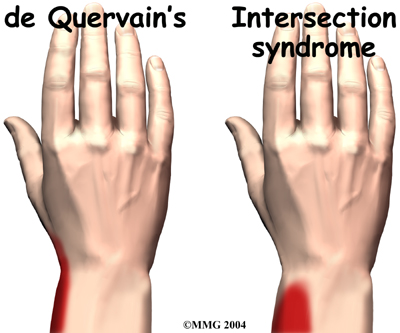
The main challenge in diagnosing this syndrome is distinguishing it from de Quervain's tenosynovitis. De Quervain's tenosynovitis is a condition that is very similar to intersection syndrome.
Both syndromes involve inflammation in the tendons of the wrist. However, the pain begins in different spots. Intersection syndrome causes pain at the intersection point, about three inches up the forearm. De Quervain's tenosynovitis causes pain along the edge of the wrist, closer to the hand. Your physiotherapist at Vernon Physiotherapy & Rehab will examine your forearm and wrist carefully to locate exactly where your pain is coming from and to ensure that the correct diagnosis is determined.
Treatment
What treatment options are available?
Nonsurgical Rehabilitation
Your initial treatment for intersection syndrome at Vernon Physiotherapy & Rehab will aim to decreasethe inflammation and pain around the area. Simply icing your wrist can often assist with the inflammation and relieve a great deal of the pain. In cases of more chronic pain, heat may be more useful. Your physiotherapist may also use electrical modalities such as ultrasound or interferential current to help decrease the pain and inflammation. Massage for the small muscles around the painful area or the larger muscles of the forearm may also be helpful at this stage.
 As this syndrome often comes on due to repetitive activity, it is most important to stop or change the activities that are causing your symptoms. Taking frequent breaks when doing repeated hand and thumb movements is also important. If possible, we will encourage you to avoid repetitive hand motions such as heavy grasping, wringing, or turning and twisting movements of the wrist. Downhill skiers may get relief by avoiding heavy planting and dragging of their ski poles and by getting a shorter pole with a smaller basket diameter which reduces the drag and force transmitted to the wrist.
As this syndrome often comes on due to repetitive activity, it is most important to stop or change the activities that are causing your symptoms. Taking frequent breaks when doing repeated hand and thumb movements is also important. If possible, we will encourage you to avoid repetitive hand motions such as heavy grasping, wringing, or turning and twisting movements of the wrist. Downhill skiers may get relief by avoiding heavy planting and dragging of their ski poles and by getting a shorter pole with a smaller basket diameter which reduces the drag and force transmitted to the wrist.
In addition to giving the wrist as much rest as possible, keeping your wrist in a neutral alignment will also assist in the healing process. In other words, keep it in a straight line with your arm, without bending it down and in. This position avoids the stress caused by stretching the tendons in this area. Your physiotherapist may even suggest the use of a splint for the area, which keeps the thumb and wrist from moving excessively and helps to keep the wrist in the neutral position. Resting for the wrist extensor tendons and the thumb muscles allows the area to begin healing.
As part of your treatment your physiotherapist may check your workstation set-up and observe the way you do your daily tasks. We will also educate you about healthy body alignment and proper wrist positions. It is our belief at Vernon Physiotherapy & Rehab that preventing future problems is as much a part of our treatment as getting rid of your existing pain.
Once the initial pain and inflammation has calmed down, your physiotherapist will focus on improving the mobility and strength of your wrist and thumb. Simple regular wrist stretching exercises will be prescribed and should be done within the limits of pain. Strengthening exercises will also be prescribed. These exercises will focus on improving both the strength of the wrist and thumb muscles, but also the ability of the hand to grip and exert force when twisting or grabbing. Exercises to improve strength will include eccentric exercises for the area. Eccentric contractions occur as the muscle lengthens and the tendon is put under stretch while resisting a force. Your physiotherapist will advise you when it is the appropriate time to start these exercises. Eccentric exercises for the wrist are done by dropping the wrist down slowly at first and then, as able, progressing to a quick motion. These exercises will put the enough stress through the injured area to start building up the tensile strength in the tissues and associated muscles. In addition to eccentric exercises, therapeutic putty might be used which adds some resistance to finger and hand motions, or simple ball gripping or handle twisting exercises may be prescribed. As you become stronger, weights or resistance bands will be used to further build up strength. Fine motor control and dexterity exercises for your thumb and hand may also be added into your rehabilitation routine depending on your occupation or the cause of your injury. If possible, we will tailor the exercises we give you to simulate the functional activities used in daily living or in your occupation.
Being that intersection syndrome is most often caused by repetitive stress in the first place, close monitoring of your rehabilitation program by your physiotherapist at Vernon Physiotherapy & Rehab is necessary to ensure excessive stress is avoided and that you do not re-injure the area during your rehabilitation.
The use of anti-inflammatory medications may be helpful to control the swelling of thetenosynovium and ease symptoms. These medications include common over-the-counter medications such as ibuprofen and aspirin or stronger prescribed medications. Your physiotherapist may suggest you see your doctor to discuss the use of anti-inflammatories or pain-relieving medications in conjunction with your physiotherapy treatment.
If rehabilitation, rest, and oral medications fail to control your symptoms, we may liaise directly with your doctor regarding their opinion on an injection of cortisone. Cortisone is a very effective anti-inflammatory medication. Cortisone injections will usually control the inflammation in the early stages of the problem, however, cortisone's effects are generally temporary, lasting from several weeks to months. This pain-free window of time, however, often allows your physiotherapist at Vernon Physiotherapy & Rehab enough time to implement rehabilitation that can cease the onset of further episodes of pain and injury.
If nonsurgical treatment is successful, you should see improvement in four to six weeks. You may need to continue wearing your splint to control symptoms. You should continue to try to do your activities using healthy body and wrist alignment and limit activities that require repeated motions of the wrist and thumb.
Vernon Physiotherapy & Rehab provides services for physiotherapy in Vernon.
Surgery
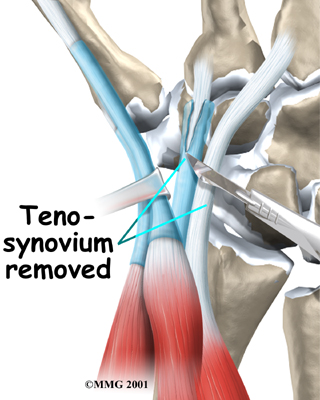
Surgery is rarely necessary to treat intersection syndrome. In extremely persistent cases, a surgeon may choose to remove some of the thickened tenosynovium around the tendons.
The operation is called a tendon release.
The tendon release procedure can usually be done on an outpatient basis, which means that you won't have to spend the night in the hospital. It can be done using a general anesthetic, which puts you to sleep, or a regional anesthetic. A regional anesthetic blocks the nerves going to only a certain part of the body. You may get an axillary block, which puts the arm to sleep, or a wrist block, which puts only the hand to sleep. It is even possible to perform the surgery by simply injecting lidocaine around the area of the incision.
During the surgery a small incision is made over the spot where the two muscles cross over the two wrist tendons. The surgeon identifies the irritated tendons, and then separates and removes the inflamed tenosynovium from the tendons. The skin is then stitched together, and your hand is wrapped in a bulky dressing. Your stitches will be removed 10 to 14 days after surgery.

Post Surgical Rehabilitation
A period of rehabilitation is needed after surgery and physiotherapy at Vernon Physiotherapy & Rehab will begin once your surgeon allows it. Your first treatment sessions will initially aim to decrease the inflammation and pain around the surgical area. Icing your wrist frequently post surgery will assist with the inflammation and relieve a great deal of the pain. Similar to the rehabilitation outlined in the non-surgical rehabilitation section above, your physiotherapist may also use electrical modalities such as ultrasound or interferential current to help decrease the pain and inflammation post surgery. Massage for the muscles of the forearm near the surgical site may also be helpful at this stage.
Simple finger movement exercises will be the first exercises we prescribe after your surgery and we will encourage them regularly throughout your day. These movements will assist with draining any swelling around the surgical site and will ensure that scar adhesions that can limit movement do not form. Gentle stretching within limits of pain will also be encouraged. Combining simple finger movements and elevation of your hand above your heart level whenever possible is a particularly effective method for draining swelling from the surgical area and hand. When your hand is down by your side, gravity causes the swelling to pool in the hand and fingers and can impede rapid recovery.
Your physiotherapist may also mobilize your wrist if your range of motion is slow to recover. This hands-on technique encourages the stiff joints to move gradually into their normal range of motion and encourages the wrist tendons to glide smoothly under the thumb muscles.
When appropriate, your physiotherapist will begin to add strengthening exercises to your rehabilitation program including gentle resistance and gripping. Again, the exercises prescribed will be similar to the exercises outlined above in non-surgical rehabilitation and will eventually include the use of some form of resistance, such as putty, weights or elastic bands, to build up the strength you will need to return to your regular activities. Post-surgical rehabilitation versus non-surgical rehabilitation may require more exercises that emphasize the fine motor control and dexterity of the hand.
As surgery is often a last resort to treat the symptoms of intersection syndrome, strict adherence to the exercise limits set by your physiotherapist as well as suggested activity modifications is crucial in order to avoid recurrence of the injury. It should be noted, that even as the injury itself heals, you might have tenderness over the incision for several months post surgery.
Generally post-surgical rehabilitation at Vernon Physiotherapy & Rehab goes very smoothly and you are able to return to your full activities over several months. If, however, during post-surgical rehabilitation your pain continues longer than it should or therapy is not progressing as your Vernon Physiotherapy & Rehab physiotherapist would expect, we will ask you to follow-up with your surgeon to confirm that the surgical area is tolerating the rehabilitation well and ensure that there are no complications that may be impeding your recovery.
Portions of this document copyright MMG, LLC.











